02.06.2026
- minute readminutes read
Oral Dysbiosis: When the Mouth's Microbial Balance Tips Towards Disease
A healthy mouth is not a bacteria-free mouth. It is a balanced one.
That distinction sits at the heart of everything oral healthcare professionals need to understand about the oral microbiome.

In the first piece, we introduced the oral microbiome as a living ecosystem and explored the systemic consequences of its disruption. Here, we go deeper: into the specific mechanisms that keep microbial communities stable, the forces that drive oral dysbiosis, and (critically) why some patients recover while others don't.
Understanding these mechanisms changes what you look for in the clinical assessment, what questions you ask, and how you frame the conversation with patients whose gum disease or caries progression doesn't follow the pattern you'd expect.
Eubiosis and dysbiosis: more than a spectrum
Eubiosis and dysbiosis explained
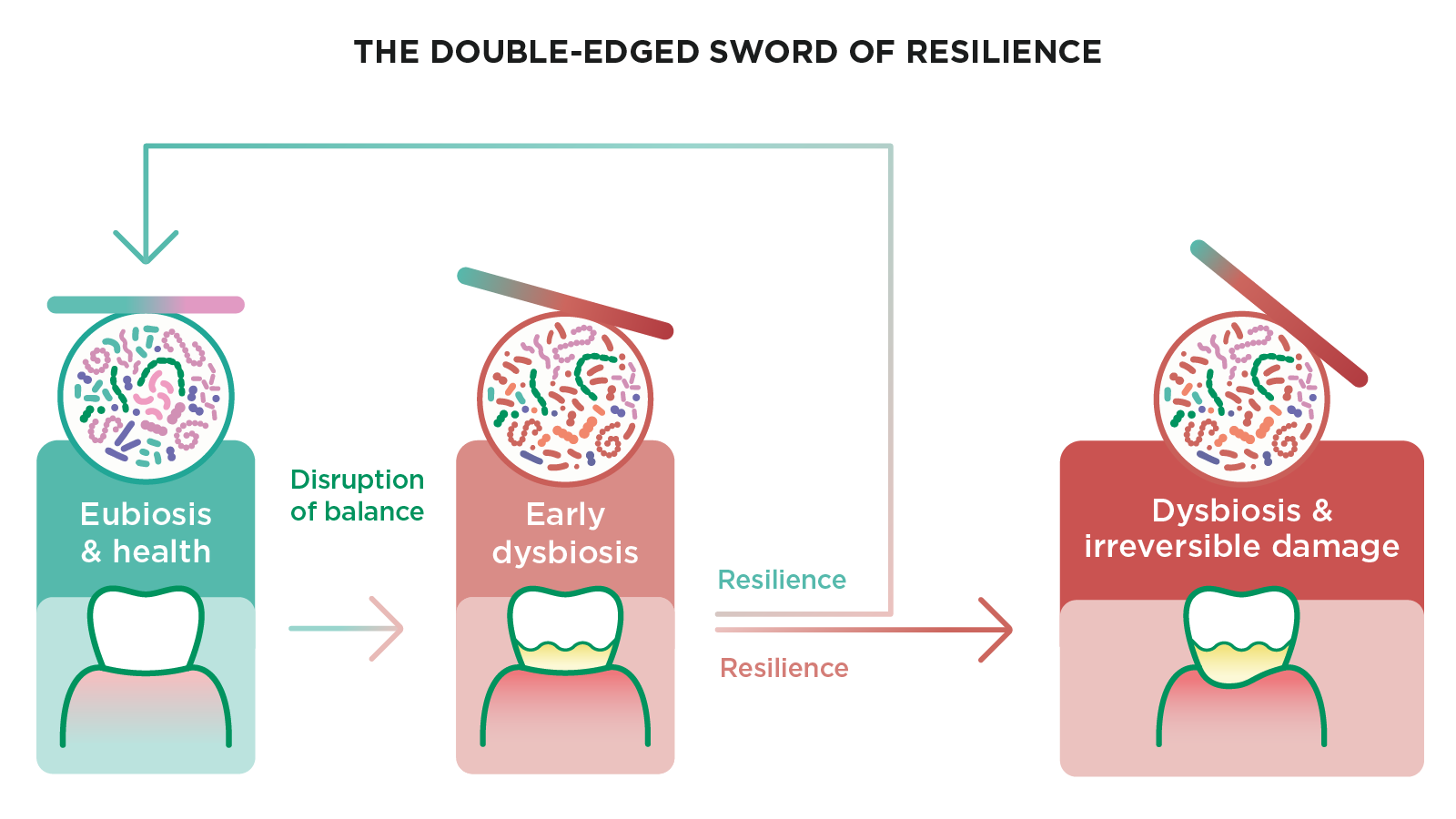
Eubiosis describes a state of beneficial microbial balance: a stable community in which beneficial bacteria and their host exist in a mutually supportive relationship.
Dysbiosis is the disruption of that balance: a state in which harmful bacteria gain dominance, microbial diversity declines, and the relationship between oral microbiota and host becomes actively harmful.
The transition between the two involves a fundamental shift in how microbial communities organise and sustain themselves.
What eubiosis actually looks like in practice
In clinical terms, eubiosis is often defined as much by what is absent as by what is present.
Healthy gingival tissue, low inflammatory markers, and a stable, non-progressive plaque community are all downstream expressions of a microbiome in balance.
What makes this balance robust is a property known as functional redundancy.
In a healthy, diverse oral microbiome, multiple bacterial species can perform overlapping ecological and metabolic functions. If one species is disrupted - for example by antibiotics, dietary changes, or other environmental stressors - other microbes can partially compensate, helping the ecosystem maintain stability.
This capacity to absorb disruption and maintain or recover equilibrium is known as microbial resilience. Importantly, resilience is not inherently beneficial: while it helps a healthy microbiome resist disturbance and return to balance, it can also stabilise dysbiotic, disease-associated communities, making them more persistent and more difficult to reverse.
How dysbiosis takes hold and why it persists

Dysbiosis is a self-reinforcing state that, once established, actively resists correction.
As pathogenic bacteria gain dominance within the oral microbiome, they begin to engineer conditions that favour their own survival. They alter the local pH, creating an environment that aciduric species thrive in and that commensals cannot tolerate.
They also compete for nutrients once used by beneficial bacteria. And through a process called quorum sensing (a cell-to-cell communication mechanism we will return to shortly), they coordinate their activity to resist host defences.
The tipping point into dysbiosis is a trap: the further the microbiome shifts towards pathogenic dominance, the harder it becomes to shift it back. This is why researchers describe a resilient dysbiotic community as one that is stable against a return to good overall health — the same property that protects a healthy microbiome can, once flipped, protect a diseased one.
The dental biofilm: protector and perpetrator
The dual nature of dental plaque
Dental plaque has long been positioned in oral health communication as something to be eliminated. The microbiome science complicates that framing significantly - and usefully.
The oral biofilm is the structural environment in which the oral microbiome lives. In its early, immature state, it is dominated by commensal streptococci and other beneficial species that actively protect against pathogenic colonisation, modulate local immune responses, and maintain the conditions necessary for microbial balance. The biofilm's existence is not the problem- its maturation is.
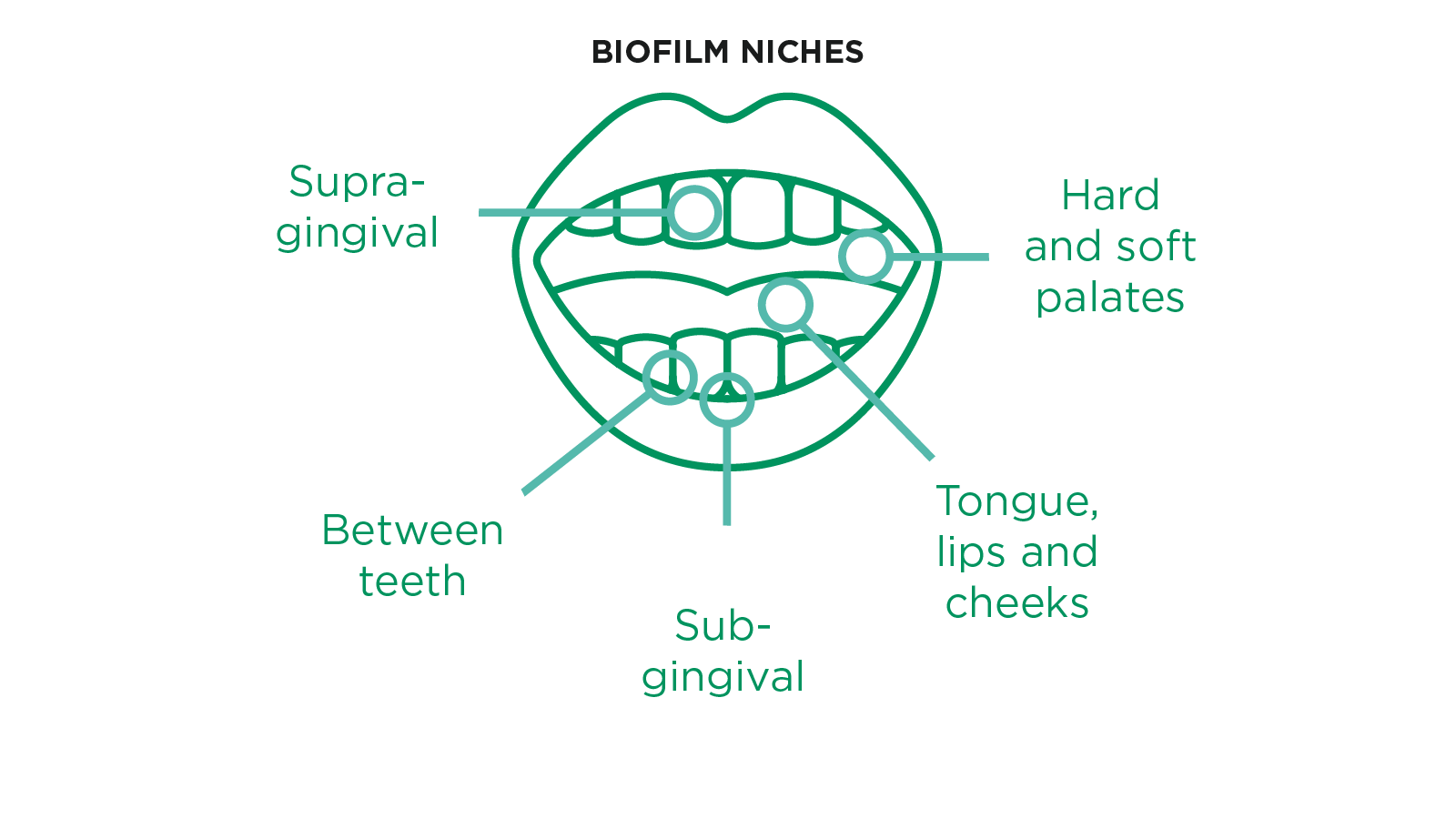
The non-shedding nature of tooth surfaces provides a uniquely stable substrate for microbial communities to establish and grow. Unlike mucosal surfaces, which shed cells continuously and limit biofilm accumulation, enamel allows communities to persist, thicken, and reorganise over time - which is precisely why teeth are where the most clinically significant dysbiotic shifts tend to occur.
The four stages of biofilm maturation and the clinical window
There are four distinct stages of biofilm development, and the clinical relevance lies in understanding where the intervention window sits.
- Stage 1 begins with the formation of the salivary pellicle - a thin protein film that coats tooth surfaces within minutes of cleaning, laying the foundation for bacterial attachment.
- Stage 2 sees early colonisers, primarily commensal streptococci, adhere to this pellicle and begin to multiply. This is the critical intervention window: the biofilm is immature, its microbial community is dominated by health-associated species, and disruption at this stage maintains the ecosystem in a balanced state.
- From Stage 3 onwards, the clinical picture changes significantly. Late-colonising species begin to arrive and establish themselves within the maturing biofilm matrix. These include anaerobic and proteolytic organisms that are closely associated with gingivitis and periodontitis.
- By Stage 4, the biofilm has reached full maturation: bacteria are released into the oral cavity, spreading the biofilm to new surfaces, and the dysbiotic community has developed the structural resilience that makes it increasingly difficult to resolve through mechanical cleaning alone.
The practical implication for oral healthcare professionals is direct: the frequency and technique of cleaning matter not simply for plaque scores, but because they determine whether the microbial community remains in its health-associated early state or progresses towards a disease-associated mature one.
Quorum sensing: how bacteria coordinate the shift
Within the biofilm, bacteria communicate through quorum sensing; a population-density-dependent signalling system that allows microbial communities to coordinate behaviour at scale. In a healthy biofilm, quorum sensing supports functional balance: bacteria regulate their own growth, resist colonisation by competitors, and adapt collectively to environmental factors.
But quorum sensing is also the mechanism by which pathogenic bacteria orchestrate the shift into oral dysbiosis. Pathogenic species use quorum sensing to delay the expression of virulence factors — the tissue-damaging, immune-evading compounds that drive periodontal destruction — until their population is large enough to overwhelm host defences.
They use it to form protective biofilm structures that resist antimicrobial agents. They adjust their metabolism to exploit nutrients from commensal bacteria and activate genes that increase antibiotic resistance.
This explains a clinical observation that many oral healthcare professionals encounter: why does periodontal disease sometimes appear to escalate rapidly, rather than progress gradually?
Because beneath the threshold of clinical visibility, the microbial community has been reorganising, and by the time clinical signs appear, the dysbiotic biofilm is already well established.
Saliva: the regulator that rarely gets enough credit
What saliva is actually doing
Saliva's contribution to oral health is typically framed in terms of moisture and lubrication. Its role in maintaining microbial balance is considerably more sophisticated than that and more clinically significant.
One of saliva's most important but least discussed functions is its role as a nutritional regulator. The nutrients it provides to oral bacteria (vitamins, glycoproteins, amino acids, urea, and bicarbonate) are largely in complex polymer forms that cannot be broken down by any single bacterial species. Processing them requires concerted interaction across multiple microbial species.
This is not incidental: by providing complex energy sources, saliva actively encourages microbial collaboration and prevents any one species from gaining a competitive nutritional advantage. It is, in effect, a structural support for microbial diversity.
Beyond nutrition, saliva delivers a continuous supply of antimicrobial proteins (including lysozyme, lactoferrin, and peroxidases) that selectively limit the growth of pathogenic species. Its bicarbonate, phosphate, and protein buffering systems counteract the acid produced by bacterial fermentation of carbohydrates, removing the acidic selective pressure that would otherwise allow aciduric species to dominate.
A well-functioning salivary system is, in microbial terms, one of the most powerful tools available for maintaining eubiosis.
When saliva fails: the clinical consequences of hyposalivation
Hyposalivation (reduced salivary flow) is a significant and underappreciated driver of oral dysbiosis in the clinical population.
Medications, anxiety, systemic disease, mouth breathing, and dehydration all reduce salivary output, with measurable microbial consequences. The buffering capacity falls. Antimicrobial protein delivery declines.
The complex nutritional matrix that supports microbial collaboration is replaced by simpler substrates that favour dominant, fast-growing, often pathogenic species. Non-oral bacteria begin to colonise surfaces that a healthy salivary environment would resist.
The clinical implication is straightforward but frequently overlooked: when a patient presents with unexplained caries progression, worsening periodontal status, or recurrent oral infection, salivary flow and quality should be included in the differential.
The connection with systemic conditions adds a further layer. Diabetes, for example, raises glucose levels in saliva and in oral tissues, altering bacterial nutrition directly and increasing susceptibility to hyposalivation. This creates a feedback loop between systemic disease and oral microbial imbalance that compounds in both directions.
The immune system: why two patients with the same habits present differently
Immune fitness as the mediating variable
As promised in the first piece of this series, this is where the immunity-as-mediator concept gets its full clinical context.
Variations in caries and periodontal disease severity can occur even under identical environmental conditions, due to differences in innate immune defence mechanisms.
In other words, two patients with comparable oral hygiene habits, similar diets, and no obvious risk factors can present with markedly different disease severity. The differentiating variable is immune fitness - the ability of the immune system to mount a proportionate, self-limiting response to dysbiotic challenge.
In patients with robust immune function, early oral dysbiosis triggers an inflammatory response that resolves the imbalance before it escalates. Beneficial bacteria are supported, pathogenic species are suppressed, and the microbiome returns to eubiosis.
In patients with compromised immune fitness, the same dysbiotic challenge produces a response that is disproportionate, self-sustaining, and ultimately destructive.
The ecological catastrophe: when inflammation feeds dysbiosis
We use the term "ecological catastrophe" to describe what happens when this cycle goes unchecked. And for good reason.
Once dysbiosis-driven inflammation becomes self-sustaining, it generates the very conditions that sustain further dysbiosis.
Increased capillary permeability opens a pathway for bacteria and their byproducts to translocate into systemic circulation, contributing to the chronic low-grade inflammation that connects oral dysbiosis to long term diseases including cardiovascular disease, diabetes, ulcerative colitis and irritable bowel syndrome.
This cycle becomes progressively harder to interrupt the longer dysbiosis persists.
Resilience: the concept that reframes disease variability
A double-edged property
Resilience, as a biological concept, is neither inherently positive nor negative. In a healthy oral microbiome, it is profoundly protective: it can absorb disruption, compensate through functional redundancy, and return to eubiosis. This is the resilience that allows the microbiome to recover from a course of antibiotics, a period of dietary change, or an acute illness.
But the same property applies to dysbiotic states. A dysbiotic microbial community, if given sufficient time and conditions to consolidate, becomes equally resilient; stable, well-defended, and resistant to restoration of balance. Dysbiosis that is allowed to mature is not simply a worsening of disease; it is the establishment of a new, entrenched microbial state that actively resists correction.
What this means at the chair
Three direct clinical implications follow from the resilience concept - each of which connects microbiome science to everyday practice:
- Disease variability between patients presenting with similar backgrounds reflects differences in immune fitness and the resilience properties of each patient's unique microbial community. Approaching unexplained disease severity through this lens opens clinical conversations that a plaque-removal model alone would not prompt.
- Chronic and refractory conditions, such as persistent periodontitis that fails to resolve after adequate mechanical therapy, may reflect a dysbiotic microbiome that has stabilised in a pathological state and developed resilience against recovery. Understanding this helps frame treatment expectations and opens the case for adjunctive approaches.
- The timing of intervention is mechanistically significant. Intervening before dysbiosis consolidates (while the biofilm is still immature and the microbial community is still capable of returning to eubiosis) is best practice, and also the point at which intervention is most effective.
Going beyond: from understanding balance to restoring it
The science of oral dysbiosis reframes the clinical mission. Oral healthcare professionals must manage a living microbial ecosystem; one whose balance determines outcomes not just in the mouth, but across the whole body.
Understanding the biofilm's dual nature, the regulatory role of saliva, the mediating function of immunity, and the double-edged property of resilience equips practitioners to intervene earlier, explain more meaningfully, and build patient understanding that goes beyond compliance into genuine health literacy.
In the next piece in this series, we explore what can actively be done to shift that balance - examining the emerging evidence for lifestyle, diet, and biological strategies as tools for moving the oral microbiome towards a more resilient eubiosis.
*This blog draws on findings from the GUM® Oral Health White Paper Series: Rethinking Oral Healthcare - Exploring the Resilience and Modulation of the Oral Microbiome (2025), developed in collaboration with Prof. Egija Zaura (ACTA, Netherlands) and Prof. Dr. Wim Teughels (KU Leuven, Belgium).
Oral dysbiosis FAQs
Oral dysbiosis does not always present with obvious symptoms in its early stages. As the microbial imbalance progresses, patients may present with persistent bad breath, bleeding or inflamed gums, increased tooth sensitivity, dry mouth, frequent mouth ulcers, or recurrent caries despite adequate brushing. Progressive gum disease that fails to stabilise with standard mechanical treatment can also indicate an entrenched dysbiotic state. These presentations are worth exploring through a microbiome lens rather than attributing solely to hygiene compliance.
Restoring microbial balance begins with re-establishing the conditions that support beneficial bacteria. Consistent mechanical disruption of the biofilm at an early stage remains the essential foundation. Beyond that, reducing dietary sugar, staying well hydrated, addressing dry mouth, managing stress, and stopping smoking all directly support a shift back towards eubiosis. In cases of established periodontal disease, professional treatment is the necessary first step before any adjunctive strategies can be effective. Emerging evidence for oral-specific probiotics and prebiotics such as xylitol, arginine, and dietary nitrate shows promise as additional tools.
Dysbiosis is generally understood to occur in three forms, which can present independently or together. The first is a loss of beneficial microbial species, reducing the diversity and functional redundancy that keeps the ecosystem stable. The second is an overgrowth of potentially pathogenic bacteria that take advantage of the resulting imbalance. The third is an overall loss of microbial diversity, leaving the ecosystem less resilient and more vulnerable to further disruption. In the oral cavity, all three patterns can contribute to conditions including caries, gingivitis, and periodontitis.
There is no fixed timeline, and this is an important expectation to set with patients. The oral microbiome can begin to shift towards a healthier composition relatively quickly with consistent mechanical cleaning and lifestyle changes - some studies show measurable microbial changes within weeks. However, where dysbiosis has become entrenched and the biofilm has matured into a resilient, pathogenic state, correction takes longer and may require professional intervention alongside behavioral change. The key clinical message is that earlier intervention produces faster, more complete results.
Eubiosis describes a state of healthy microbial balance in the mouth, where a diverse community of beneficial bacteria maintain appropriate checks on potentially harmful species. Dysbiosis is the disruption of that balance - a shift in which pathogenic bacteria dominate, microbial diversity declines, and the relationship between the microbiome and its host becomes harmful rather than supportive. Critically, dysbiosis is not simply a passive consequence of neglect. Once established, it can become self-sustaining, making restoration of eubiosis progressively more difficult without intervention.
Saliva is one of the most important regulators of oral microbial balance. It delivers antimicrobial proteins that limit pathogenic overgrowth, maintains a neutral pH that prevents acid-tolerant species from dominating, and provides complex nutritional substrates that require microbial collaboration to break down. Saliva actively supports diversity. Reduced salivary flow significantly increases the risk of dysbiosis and is associated with higher rates of caries, periodontal disease, and oral infection. Medications, stress, systemic conditions such as diabetes, and dehydration are all common causes worth exploring in the clinical assessment.
Yes - and this is one of the most clinically significant aspects of oral microbiome science. When oral dysbiosis is sustained, the resulting chronic inflammation does not remain contained to the mouth. Bacteria and their byproducts can translocate into systemic circulation, contributing to low-grade systemic inflammation that has been associated with cardiovascular disease, type 2 diabetes, inflammatory bowel disease, and other chronic conditions.
Quorum sensing is the cell-to-cell communication system that bacteria within the oral biofilm use to coordinate their behavior. In a healthy biofilm, it supports balance and helps commensal species resist colonisation by pathogens. In a dysbiotic one, pathogenic bacteria exploit quorum sensing to delay the release of tissue-damaging virulence factors until their numbers are sufficient to overwhelm host defences - which is why periodontal disease can appear to escalate rapidly once it takes hold. It also explains why bacteria within a mature biofilm can develop tolerance to antimicrobial agents, including those found in mouthwashes.
Related Articles
-
How Oral Microbiome Resilience Is Reshaping Prevention and Care - Let's Talk Oral Health Explore how resilience in the human oral microbiome is reshaping prevention, periodontal care, and long-term oral and systemic health.
-
The Oral Microbiome: What Every Dentist Needs to Know The oral microbiome is reshaping our understanding of oral and systemic health. Discover what the science means for your patients and your practice.

-
Gut and Oral Microbiomes: Their Impact on Overall Health Learn about the connection between the gut and oral microbiomes and their impact on overall health. Key insights for patient care.

-
Oral Health and Overall Health: Their Impact on Each Other Discover evidence-based behavioral change strategies for preventing oral diseases.

-
Physical Activity and Periodontitis: Effects on Oral Microbiome Explore the evidence linking physical activity to periodontitis, including effects on periodontal health, systemic inflammation, and oral microbiome composition

-
Lifestyle Medicine and Oral-Systemic Health - Let's Talk Oral Health In this second episode, Dr. Crystal Marruganti explores multimorbidity and how lifestyle and behavior shape outcomes.

-
The Oral Microbiome in Health and Disease Discover how managing the oral microbiome can be an effective tactic in a 360° strategy to prevent periodontal and peri-implant diseases.

-
Oral Microbiome Management: A Guide for Dental Professionals Why do some patients keep relapsing? Explore how oral microbiome management, probiotics for oral health, and biological modulation are changing dentistry.

-
Oral Microbiome Balance: A Maintenance Guide for Hygienists Plaque removal is just the start. Learn how hygienists can maintain oral microbiome balance through biofilm management, lifestyle advice, and probiotics.

-
Probiotics in Pregnancy Hormonal changes during pregnancy can easily lead to gingivitis or periodontitis. Probiotics are a safe and effective adjunct in the management of gum disease.

-
Probiotics and Dentistry: Key Facts and Findings While research into the oral microbiome is ongoing, the early indications about probiotic benefits are as promising as the prospects.
-
Probiotics Reduce Candida Albicans in Elderly Patients Learn about the unique oral health risks faced by older adults, including candidiasis, and the factors contributing to increased susceptibility.

-
The Effect of Probiotics for Oral Health: Cleaning Up Infections The latest scientific evidence shows that the probiotic Lactobacillus reuteri Prodentis (contained in GUM® PerioBalance®) supports the health of gums and teeth.

-
Lactobacillus reuteri Prodentis, Probiotic for Maintenance of Healthy Gums Multiple studies confirm that Lactobacillus reuteri Prodentis contained in GUM PerioBalance has plaque inhibition, anti-inflammatory, and antimicrobial effects.
-
Probiotics and Their Use in Peri-Implant Mucositis Can probiotics help with peri-implant mucositis? Two highly promising studies show that probiotic can bring to a significant improvement in clinical parameters.

-
What Today’s Dental Professionals Should Know About Oral Microbiome The oral microbiome is a keen area of research today, owing heavily to its role in periodontal disease as well as systemic health conditions.
-
Stress and Oral Health: Implications of Chronic Stress As mounting evidence points to chronic stress as a clear risk indicator for periodontal disease, dental professionals should get proactive in addressing it.

-
Oral Health and Rheumatoid Arthritis: Key Facts and Findings The dental community should be aware of growing evidence around the links between oral health and rheumatoid arthritis.

-
How Lifestyle Factors Affect Periodontal Disease If your patients have questions about how their lifestyle may affect their risk of developing periodontal disease, this is reliable information you can provide.

-
How Inflammatory Bowel Diseases Increase Oral Health Risk Patients suffering from IBDs are at an increased risk of developing periodontitis because the diseases modify their oral microbiota and inflammatory processes.

-
Delivering Innovative Oral Care for Your Dental Patients How can dental professionals take advantage of the latest technology, research, and best practices to provide cutting-edge service for their patients?

-
Educate Patients on Proper Gum Care for Diabetes Control The benefits of oral hygiene go beyond tooth and gum health. Patients need to understand how gum disease can affect conditions like diabetes and vice versa.

-
Understanding the Role of Oral Bacteria in Colorectal Cancer Data from research around the role of F. nucleatum in the progression of colorectal cancer is too striking for dental professionals to ignore.
