
03.07.2026
- minute readminutes read
Oral Microbiome Management: A Clinical Framework for Dentists
It's not uncommon for patients whose risk of persistent periodontal disease stays stubbornly high despite following treatment plans, maintaining good oral hygiene, and attending regular check-ups. Emerging research into the oral microbiome is providing dental professionals with better management techniques.

Research into the dental microbiome is giving practitioners a clearer framework for understanding why some patients continue to struggle, and how treatment strategies can be adapted more effectively.
In the first two installments, we explored the science behind the oral microbiome: what it is, how it shifts between balance and dysbiosis, and why microbial resilience plays such an important role in long-term oral health.
Here, we take a closer look at how oral microbiome management can be applied in day-to-day clinical practice.
When good treatment is not enough
Reframing caries and periodontitis as dysbiosis-driven disease
The conventional model positions periodontitis as a disease caused by bacteria. The microbiome model is more precise: they are diseases caused by an ecological imbalance. Bacteria are the mechanism, but dysbiosis is the underlying condition.
This distinction changes the treatment question. Reducing bacterial load addresses the immediate presentation, but if the conditions that produced the dysbiotic shift remain in place, the pathogenic community will re-establish itself in the cleared space. The biofilm regrows within hours of cleaning. Without the microbial environment that favours commensal dominance, recurrence is not a question of compliance.
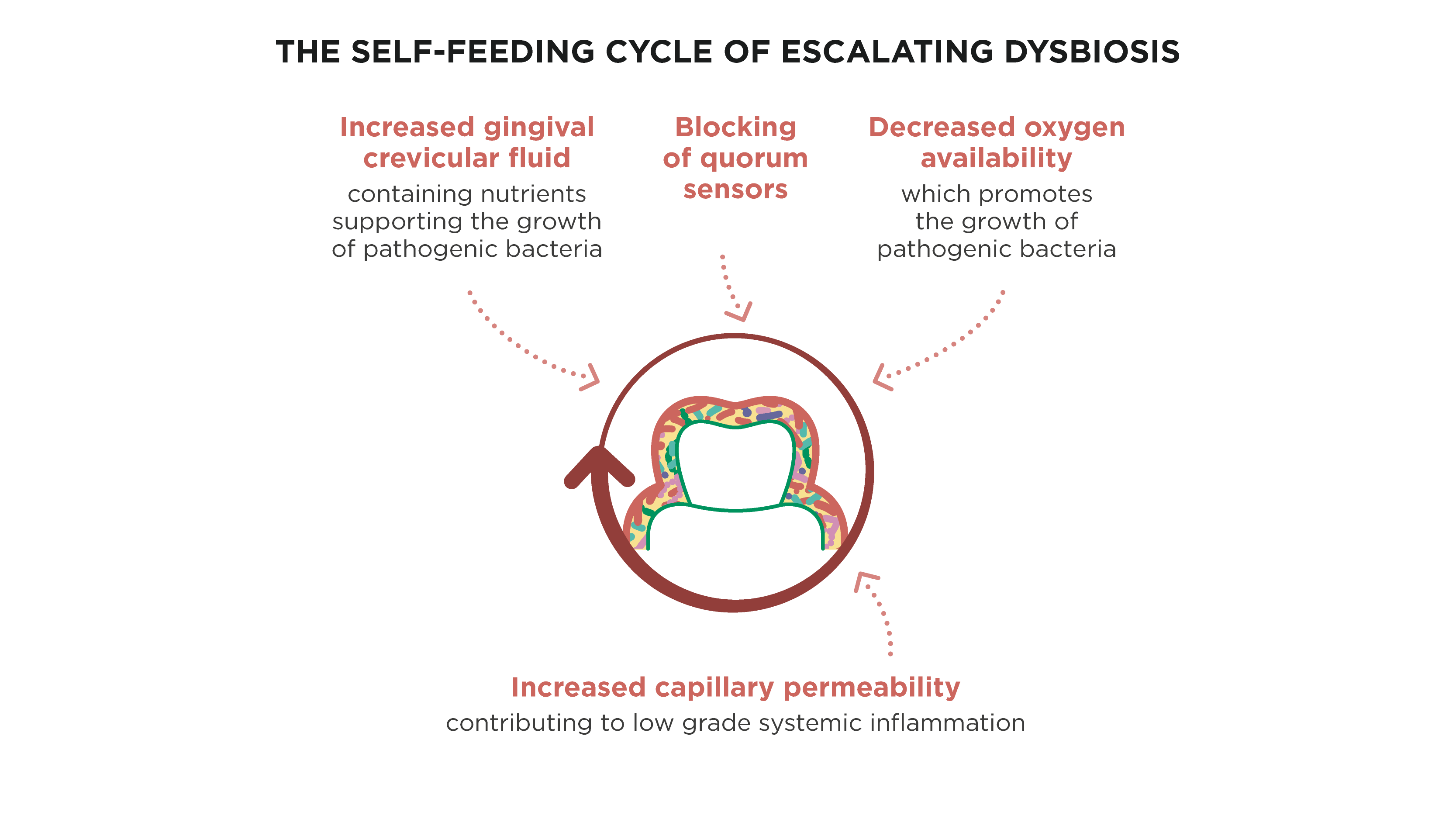
It is a question of ecology. Research published in the Journal of Oral Microbiology puts this plainly: manipulating the diseased oral microbiome requires strategies that go beyond bacterial suppression towards active restoration of a balanced microbial community.
The clinical question is how to do that, and when.
Three levels of oral microbiome management
Oral microbiome management can be broadly thought of at three levels. Most dental care already addresses the first two. The third is where the research (and clinical interest) is increasingly heading.
Level 1: mechanical control
Mechanical disruption of the biofilm remains the foundation of effective oral care. Scaling, root planing, and consistent home hygiene help keep the microbial community in a healthier, less mature state. No adjunctive treatment replaces this. Everything else works best when good mechanical control is already in place.

Level 2: chemical risk reduction
Antimicrobials, chlorhexidine, fluoride, and essential oil mouthwashes all have an important role in reducing bacterial load and managing specific clinical situations, such as acute infections, post-surgical care, or periods of increased risk.
But their limitations are well recognised. Most antimicrobial agents are non-selective, affecting both good and bad bacteria. Mature biofilms are also inherently resistant, and repeated exposure can encourage bacterial tolerance through mechanisms such as quorum sensing.
These products remain useful and clinically appropriate, but they were developed to control bacterial challenge, not necessarily to restore balance within a dysbiotic oral ecosystem.
Level 3: biological modulation
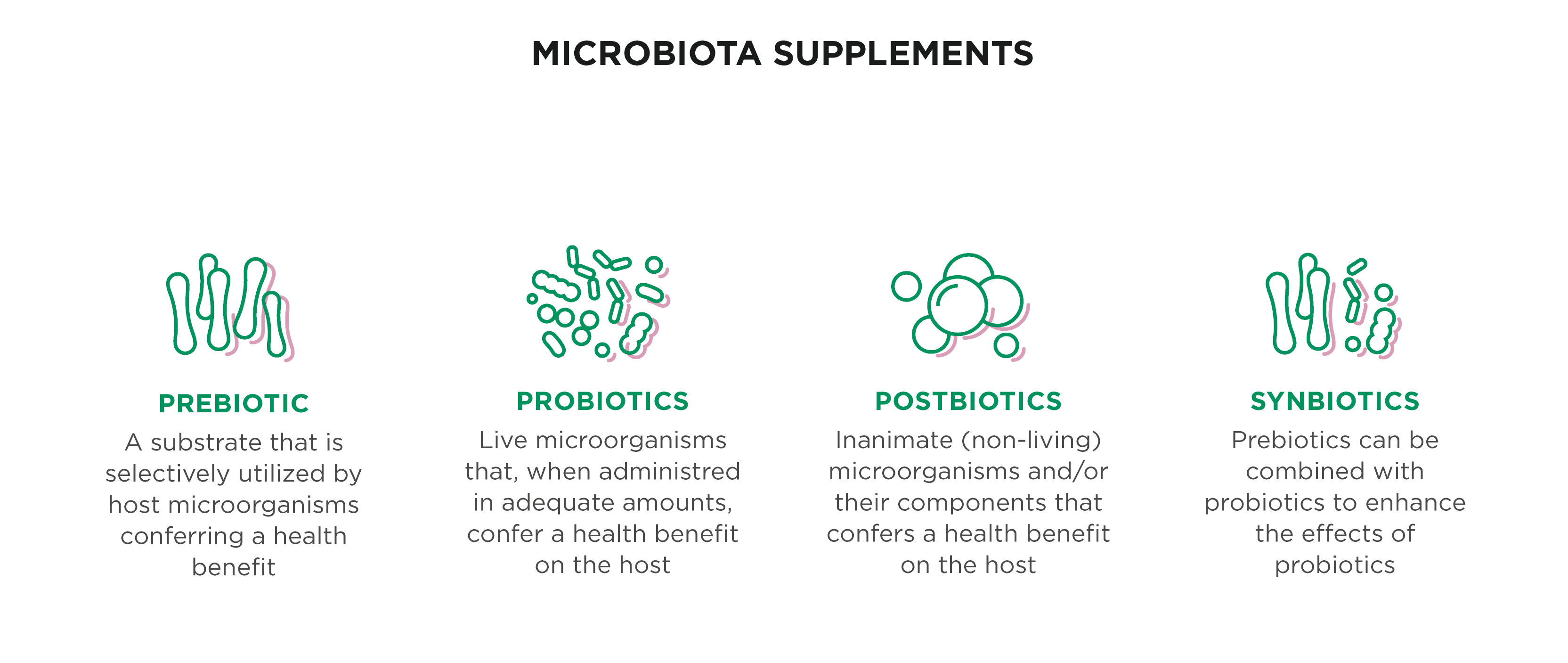
This is the area now attracting growing attention. Biological modulation aims to positively influence the oral environment, using prebiotics, probiotics, postbiotics, and synbiotics to encourage a healthier microbial balance rather than simply suppressing bacteria.
The evidence base is still evolving, and universal clinical guidelines are not yet established. Even so, there is now enough meaningful research to support informed use in selected patient groups, and the body of evidence continues to grow.
Prebiotics for oral health: shifting the environment
Simply put, prebiotics are the nutrition for good bacteria. They work by changing the oral environment in ways that favour beneficial bacteria while making conditions less supportive for pathogenic species. A recent review highlighted three oral prebiotics with some of the strongest evidence to date: xylitol, arginine, and nitrate.
Xylitol is already familiar to many clinicians. It has been shown to reduce salivary Streptococcus mutans levels, increase plaque pH, and support remineralization. The evidence is particularly relevant for caries-active patients. That said, its effectiveness can be reduced when diets remain high in fructose and sucrose, so dietary advice still matters.
Arginine works differently. It is metabolized through the Arginine Deiminase System, producing ammonia that helps neutralize plaque acids. By reducing acidity, it removes some of the selective pressure that allows acid-tolerant species to dominate. There is also evidence suggesting arginine works well alongside fluoride, making it a sensible addition to existing preventive strategies for high caries-risk patients rather than a replacement for them.
Nitrate, found naturally in foods such as beetroot, spinach, and leafy greens, is converted by oral bacteria into nitric oxide. Nitric oxide has antimicrobial effects against anaerobic bacteria associated with oral disease. Research suggests dietary nitrate may help suppress periodontal pathogens, maintain a healthier plaque pH, and support a more balanced dental microbiome overall. An added benefit is that nitric oxide is also linked with improved vascular function through vasodilation, which may be relevant for patients with broader cardiovascular risk factors.
Probiotics for oral health: introducing beneficial strains
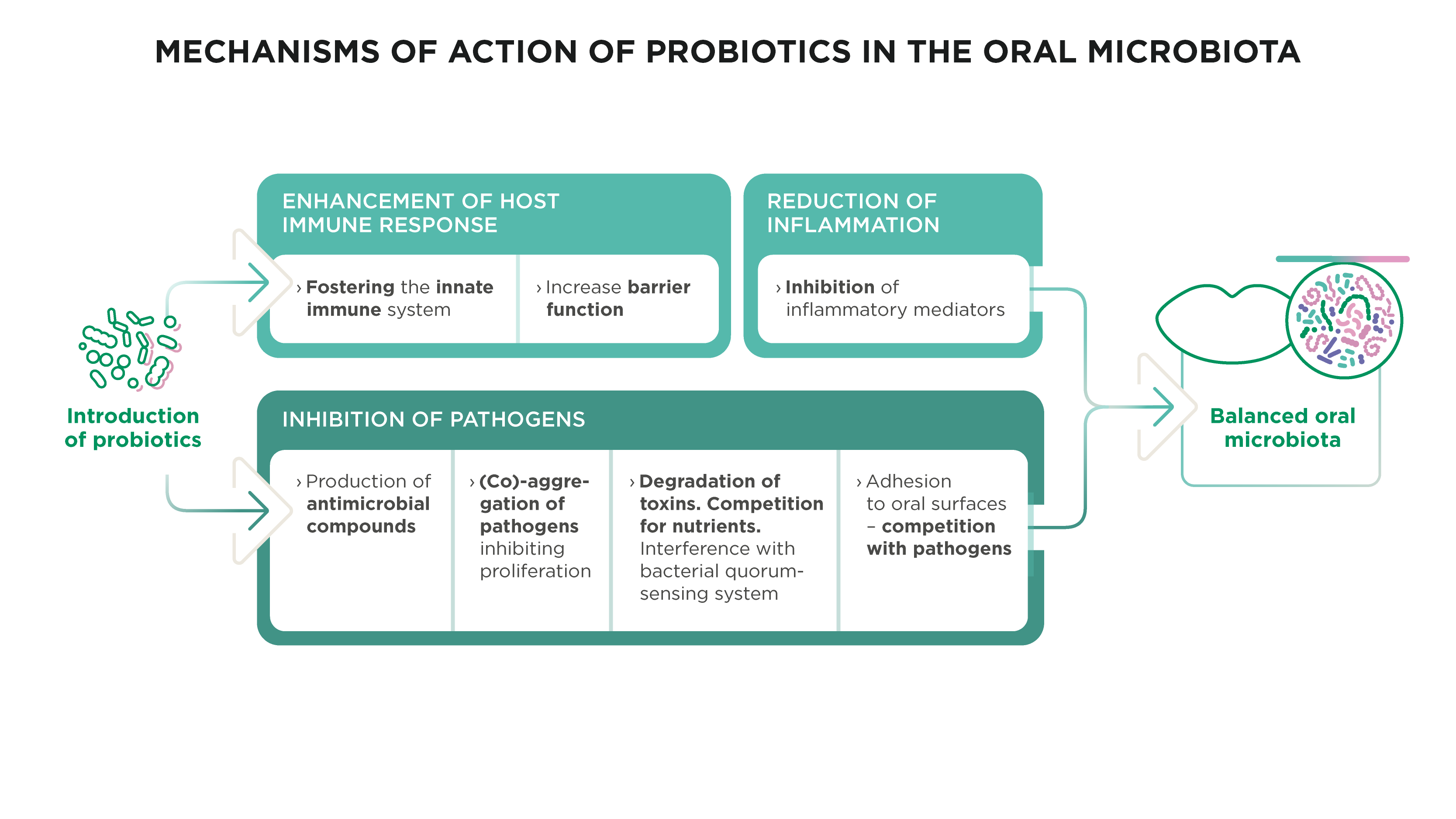
Oral probiotics work by introducing live microorganisms that can compete with pathogenic bacteria, produce antimicrobial compounds, influence the local immune system response, and help strengthen the mucosal barrier.
For patients asking about probiotics to support the oral microbiome, the key point is that not all probiotics work in the same way, and the specific strain matters far more than many people realize.
Strain specificity
One reason earlier probiotic studies produced mixed results is that many used strains originally developed for gut health rather than the oral environment. Strains such as Lactobacillus rhamnosus GG are well researched in gastrointestinal medicine, but they do not consistently colonise or persist within the mouth.
More recent research has focused on oral-specific strains that are naturally better suited to the microbial niches found in the oral cavity. These appear to produce more targeted and reliable outcomes. A 2024 review provides a detailed overview of the current strain landscape and is a useful resource for clinicians considering evidence-based recommendations.
The current evidence
Limosilactobacillus reuteri is currently the most widely studied oral-specific probiotic strain. Research has linked it with improvements in periodontal inflammation, reductions in caries-associated bacteria, lower Candida prevalence, and improvements in halitosis.
A systematic review and meta-analysis found that probiotics used alongside scaling and root planing resulted in statistically significant improvements in periodontal outcomes compared with mechanical treatment alone. There is also growing interest in their use as adjuncts in peri-implant mucositis management, particularly given the practical limitations of mechanical cleaning around implant surfaces.
Timing also appears to play an important role. Introducing probiotics into an established dysbiotic biofilm means they are competing against a mature and resilient pathogenic community. Following thorough professional debridement, however, those same strains are more likely to colonise successfully and persist. In other words, the sequence of treatment may be just as important as the probiotic itself.
Synbiotics: enhancing colonisation and effect
Synbiotics combine a probiotic strain with a prebiotic substrate designed to support its growth and persistence. Put simply, the probiotic is introduced into an environment that is already better suited to its survival, improving the chances of successful colonisation and longer-lasting effects.
In the oral setting, the combination of glycerol with L. reuteri currently has some of the strongest supporting evidence. Research found that pairing the two significantly enhanced probiotic activity within oral biofilm compared with L. reuteri alone.
Synbiotic therapy is still an emerging area of dentistry, but it offers a sensible progression for patients who have already tried probiotic adjuncts without seeing consistent results. By supporting both the introduced bacteria and the surrounding environment, the combined approach may provide more stable and clinically meaningful outcomes over time.
Deciding when to go to level 3
Biological modulation should not replace good mechanical care, but rather support it. Particular value may lie in both supporting patients with persistent microbial imbalance despite appropriate treatment and in helping maintain a healthier, more resilient oral microbiome over the long term.
Recurrent periodontitis
Some patients continue to relapse even after thorough scaling, regular maintenance, and reasonable compliance. In these cases, the issue may be less about hygiene failure and more about a dysbiotic microbiome that has become resilient and difficult to shift. Biological adjuncts used alongside retreatment may help target that underlying imbalance more directly.
Elevated caries risk without obvious hygiene failure
Likewise, there are patients who remain at high caries risk despite good oral hygiene and appropriate fluoride use. In these situations, prebiotics aimed at improving plaque pH and reducing acidogenic bacterial dominance may offer a more targeted approach than simply increasing conventional chemical interventions.
Maintenance phase support
Following periodontal treatment, the goal is not only to remove disease but also to maintain a stable, health-associated microbial environment. Biological adjuncts may help slow pathogenic recolonisation between appointments and support the long-term stability achieved through mechanical therapy.
Peri-implant care
Peri-implant maintenance is another area where biological modulation may have value, particularly in patients with a previous history of periodontitis. The microbial risk profile in these patients is already established, and mechanical access around implant surfaces can be challenging, making adjunctive strategies worth considering.
Medically complex patients
Patients with conditions such as diabetes, cardiovascular disease, or immunosuppression are often more susceptible to dysbiosis because of altered immune function. In these cases, supporting oral microbial balance may have implications beyond oral health alone and may contribute to the wider management of systemic health risks.
Closing the loop: a microbiome-informed framework
The framework outlined here is not a departure from conventional dentistry, but a natural extension of it. It provides a way of thinking about the patients who don’t always respond predictably to standard approaches, despite appropriate treatment and maintenance.
The direction of current research is clearly moving towards more microbiome-informed protocols. In time, this is likely to mean a more individualized form of risk assessment that considers microbial profile, salivary function, immune status, and systemic health alongside the traditional clinical indicators used today.
Routine microbial profiling is not yet part of everyday practice, but the tools described at Level 3 already exist and can be used now in selected cases. Importantly, the patient groups most likely to benefit from these approaches are already identifiable within routine clinical work.
This article draws on findings from the GUM® Oral Health White Paper Series: Rethinking Oral Healthcare - Exploring the Resilience and Modulation of the Oral Microbiome (2025), developed in collaboration with Prof. Egija Zaura (ACTA, Netherlands) and Prof. Dr. Wim Teughels (KU Leuven, Belgium).
Oral microbiome management FAQs
Periodontal disease recurs because successful mechanical treatment removes the immediate bacterial challenge without necessarily restoring the microbial conditions that prevent pathogenic bacteria from re-establishing. The oral biofilm regrows within hours of cleaning, and in patients whose oral environment remains dysbiotic, the same disease-associated bacterial species quickly regain dominance. Biological modulation strategies, including oral probiotics and prebiotics, are increasingly being explored as adjuncts to address this underlying microbial instability.
Strain specificity is the critical factor. Gut-derived strains do not reliably colonize the oral environment, which explains the inconsistent results in earlier trials. Oral-specific strains, particularly Limosilactobacillus reuteri, have the strongest evidence for oral applications, with demonstrated effects on periodontal inflammation, caries-associated bacteria, and Candida prevalence. Timing matters too: probiotics are most effective when introduced after professional debridement, when space in the biofilm has been cleared.
Prebiotics for oral health are substrates that selectively feed beneficial bacteria, modifying the oral environment to limit pathogenic growth. The three with the strongest evidence are xylitol, which reduces Streptococcus mutans and raises plaque pH; arginine, which counteracts plaque acidification; and dietary nitrate, found in beetroot and leafy greens, which converts to nitric oxide with antimicrobial activity against anaerobic periodontal pathogens.
Yes, with an important caveat: they work best as an adjunct to conventional treatment, not a replacement for it. A systematic review and meta-analysis found that probiotic therapy combined with scaling and root planing produced measurable improvements in clinical periodontal parameters compared with mechanical treatment alone. Early evidence also supports their use in peri-implant mucositis management.
A probiotic introduces live beneficial bacterial strains that compete with pathogens and modulate the immune response. A prebiotic is a substrate that feeds beneficial bacteria already present in the teeth and gums, shifting the environment in their favor. A synbiotic combines both, pairing a prebiotic substrate with a probiotic strain to improve colonization, persistence, and clinical effect.
Consistent mechanical biofilm disruption is the foundation. Beyond that, prebiotics such as xylitol, arginine, and dietary nitrate can shift the plaque environment away from conditions that favor pathogenic species. Oral-specific probiotic strains, introduced after professional debridement, can help re-establish microbial balance. Diet, hydration, stress management, and smoking cessation all have measurable effects on microbial composition and are worth addressing alongside clinical treatment.
Biological modulation uses prebiotics, probiotics, and synbiotics to actively restore and maintain a balanced oral microbial community. It sits alongside mechanical and chemical approaches as the third level of oral microbiome management, and is most relevant in patients with recurrent disease, high caries risk, peri-implant concerns, or systemic health issues that increase susceptibility to dysbiosis.
Diet is the most significant lever. Fibre-rich foods and nitrate-containing vegetables such as beetroot and spinach feed health-associated bacteria, while reducing sugar removes the acidic conditions that allow pathogenic species to dominate. Staying well hydrated supports salivary flow, one of the most important natural regulators of microbial balance. Consistent brushing and interdental cleaning prevent the biofilm maturing into a dysbiotic state. Stopping smoking, managing stress, and adequate sleep all support the immune fitness that keeps the microbial community stable. For patients where lifestyle measures alone are insufficient, oral-specific probiotics and prebiotics such as xylitol and arginine offer an evidence-based adjunct.
Related Articles
-
Physical Activity and Periodontitis: Effects on Oral Microbiome Explore the evidence linking physical activity to periodontitis, including effects on periodontal health, systemic inflammation, and oral microbiome composition
-
Lifestyle Medicine and Oral-Systemic Health - Let's Talk Oral Health In this second episode, Dr. Crystal Marruganti explores multimorbidity and how lifestyle and behavior shape outcomes.

-
Oral Microbiome Management: A Guide for Dental Professionals Why do some patients keep relapsing? Explore how oral microbiome management, probiotics for oral health, and biological modulation are changing dentistry.