
13.08.2021
- minute readminutes read
Lactobacillus Reuteri Prodentis, Probiotic for Maintenance of Healthy Gums
Periodontal disease is among the most common of human diseases, arising due to an imbalance between pathogenic bacteria and desirable or beneficial microorganisms. The susceptibility of the host also plays a significant role and can be influenced by a range of circumstances, dietary and lifestyle choices, or diseases.
Initial therapy for periodontal diseases focuses on reducing the number of unwanted pathogens through scaling and root planing (SRP). For these same patients, numerous studies confirm that the probiotic bacteria Lactobacillus reuteri Prodentis (LrP), represents a useful therapeutic supplement in anti-infective therapy, and for periodontal maintenance therapy post intervention.
Studies also show that some bacteria have both anti-microbial and anti-inflammatory properties. The aim of treatment with Lactobacillus reuteri Prodentis is to sustainably increase the proportion of beneficial bacteria in the oral cavity and to restore the natural balance of the oral flora.
Antimicrobial, anti-inflammatory, and plaque inhibitory effects of Lactobacillus reuteri Prodentis are confirmed in multiple studies.
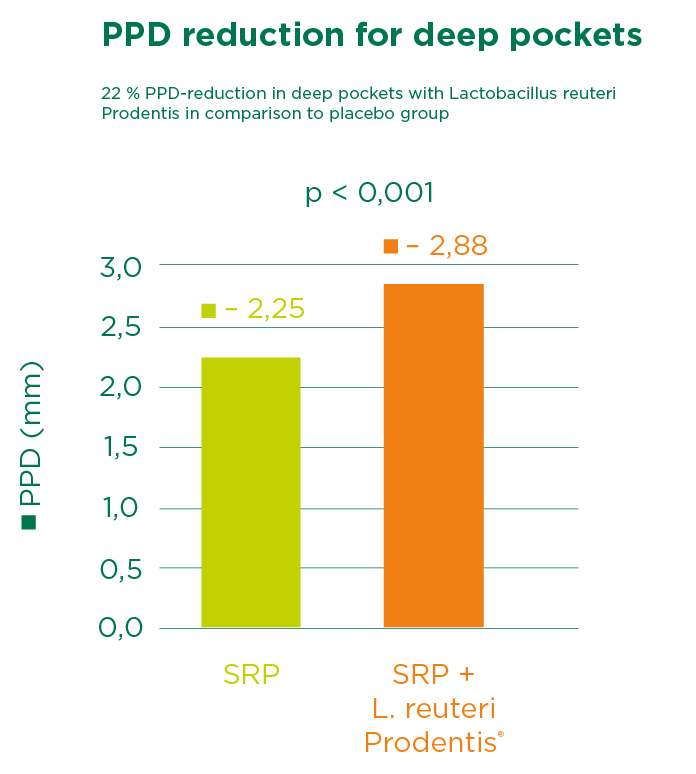
In the study by Teughels et al. 30 chronic periodontitis patients were recruited and monitored clinically and microbiologically at baseline, 3, 6, 9 and 12 weeks after therapy. All patients received one-stage full-mouth disinfection and were randomly assigned over a test (SRP + probiotic, n = 15) or control (SRP + placebo, n = 15) group. The lozenges were used two times a day for 12 weeks.
The result shows that the patient group receiving Lactobacillus reuteri Prodentis had significantly fewer patients with deep pockets. A significant reduction in the pocket depth of deep pockets as well as an attachment gain were also observed, and the pathogenic germ Porphyromonas gingivalis was significantly more contained (- 1.17 cfu/ml vs. - 0.22 cfu/ml in saliva after 12 weeks).
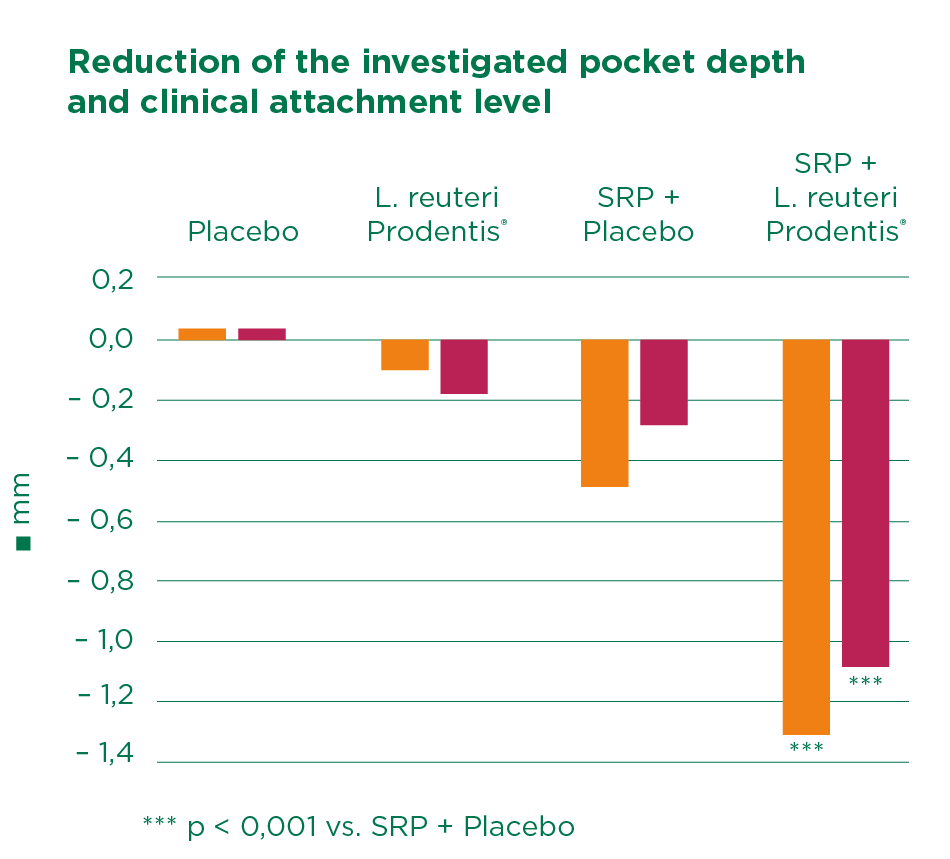
The double-blind study by Vivekananda et al. confirms these results. Half of the 30 periodontitis study participants were treated with SRP, while the other served as control.
From day 21 to 42, one group received two tablets of Lactobacillus reuteri Prodentis per day, and the other group a placebo. In all treated patients, the plaque index (PI), the gingiva index (GI) and the gingiva bleeding index (GBI) improved significantly, although to differing levels.
While the most significant effect was observed with combination of SRP and Lactobacillus reuteri Prodentis, the combination of SRP plus placebo actually produced worse results than treatment with Lactobacillus reuteri Prodentis alone.
In patients treated with SRP plus Lactobacillus reuteri Prodentis, pocket depth was reduced from 5,08 to 3,78 mm and the clinical attachment level was reduced from 3,93 to 2,85 mm.
The study confirmed the plaque inhibition, anti-inflammatory, and antimicrobial effects of Lactobacillus reuteri Prodentis. The authors concluded that considering the beneficial effects of probiotics, this therapy could serve as a useful adjunct or alternative to periodontal treatment when SRP might be contraindicated.
Martin Cabezas and colleagues undertook a meta-analysis at the Osteoarticular & Dental Regenerative Nanomedicine unit at INSERN in Strasburg, France. The co-authors included Randomized controlled trials (RCTs) comparing SRP + probiotic versus SRP alone. This work confirmed the beneficial effects of probiotic treatment and supports the adjunctive use of Lactobacillus reuteri Prodentis to SRP in chronic periodontitis treatment, especially for patients with deep pockets.
Have a look at further study results from various risk groups: The influence of our diet on periodontitis, Probiotics reduce Candida albicans in elderly patients, Probiotics in pregnancy and Probiotics and their use in peri-implant mucositis.
[1] Teughels et al. (J Clin Periodontol) 2013, 1025–35.
[2] Vivekananda, et al. (J Oral Microbiology 2010, 2; 5344-ff).
[3] Rodrigo Martin-Cabezas, et al. (J of Clinical Periodontology 2016; 520-530).
Related Articles
-
Probiotics in Pregnancy Hormonal changes during pregnancy can easily lead to gingivitis or periodontitis. Probiotics are a safe and effective adjunct in the management of gum disease.
-
Probiotics and Dentistry: Key Facts and Findings While research into the oral microbiome is ongoing, the early indications about probiotic benefits are as promising as the prospects.
-
Probiotics Reduce Candida Albicans in Elderly Patients Learn about the unique oral health risks faced by older adults, including candidiasis, and the factors contributing to increased susceptibility.

-
The Effect of Probiotics for Oral Health: Cleaning Up Infections The latest scientific evidence shows that the probiotic Lactobacillus reuteri Prodentis (contained in GUM® PerioBalance®) supports the health of gums and teeth.

-
Probiotics and Their Use in Peri-Implant Mucositis Can probiotics help with peri-implant mucositis? Two highly promising studies show that probiotic can bring to a significant improvement in clinical parameters.

-
What Today’s Dental Professionals Should Know About Oral Microbiome The oral microbiome is a keen area of research today, owing heavily to its role in periodontal disease as well as systemic health conditions.
-
Gut and Oral Microbiomes: Their Impact on Overall Health Learn about the connection between the gut and oral microbiomes and their impact on overall health. Key insights for patient care.

-
Ulcerative Oral Mucosa Lesions: Manifestations and Categories Oral mucosal lesions (aphthous ulcers) are acute, painful, whitish-yellow, fibrinous mucosal defects a with red halo. Here described their classification.

-
The Value of Saving Teeth vs. Dental Implants The value of saving teeth goes beyond dollars and cents. Regeneration paves the way for patient trust and better oral care opportunities.

-
Root Caries: Helping Patients Understand and Manage Helping patients understand what root caries are, and how to prevent them, is increasingly vital for dental pros as the global elderly population grows.

-
Probiotic Health Maintenance of the Gums Periodontal diseases arise due to a mismatch between existing pathogenic bacteria and desirable beneficial germs.
-
New EFP Guidelines for Stage IV Periodontitis The EFP recently released evidence-based, interdisciplinary guidelines for treating stage IV periodontitis. Here’s what professionals should know.

-
Chlorhexidine, the Gold Standard in Dentistry, Mode of Action Chlorhexidine is one of the main antibacterial ingredients in oral care products as GUM® PAROEX®, its antibacterial activity can last for more than twelve hours.

-
How to Motivate your Patients to Use Interdentals It may be difficult for the patient to change habitual behaviors and implement your recommendations immediately. Discover how.
-
Delivering Innovative Oral Care for Your Dental Patients How can dental professionals take advantage of the latest technology, research, and best practices to provide cutting-edge service for their patients?

-
Interdental Cleaning, Extremely Important, but Still Underestimated Interdental cleaning is important. It's proven that rubber interdental cleaners, such as GUM® SOFT-PICKS®, provide optimal cleaning and increased compliance.
